
The light of rejection-free, healthy kidney transplants has entered the tunnel, and should arrive at our end in just three to five years.
Last month a senior researcher from the Cell and Tissue Therapies WA at the Royal Perth Hospital (CTTWA) presented a paper to the Renal Society of Australia‘s annual conference that has profound implications for us BigDers. It detailed their early clinical trial successes in using Mesenchymal Stem Cells (MSCs) to stop kidney transplant rejection and to repair acute kidney injury (among many other medical wonders).
Quick MSC primer:
Stem cells in our bodies have the amazing ability to self-renew (make exact copies of themselves) as well transform, or differentiate, into other cell types with specialized functions, such as blood cells, muscle cells, and so on. They become the various cells throughout our bodies during early development, and help maintain and repair certain tissues during growth and adulthood.

MSC Manufacture
Mesenchymal (“Mezen-kye mel”) Stem Cells are adult stem cells that can give rise to many types of tissue, such as bone, cartilage and fat. MSCs were originally discovered in bone marrow, but they also exist in other body tissues, including skin, fat, placenta and umbilical cord blood.
In the mid-2000s, early clinical trials found MSCs could suppress inflammation and repair damaged tissue, and might potentially be used to treat diseases like myocardial infarction, liver cirrhosis, Crohn’s disease and amyotrophic lateral sclerosis (ALS).
Then in 2006, researchers found that they could also help repair damaged tissue, suppress immune reactions and even prevent rejection. Not just for matched donor-recipients, but for universal use: they induce no immune response of their own so they can be manufactured, frozen and provided at call, off the shelf.
Successes with transplants
CTTWA at Royal Perth Hospital, like many others around the world, began working with MSCs around 2005. Initially, they developed processes and techniques to manufacture them (they are now a licenced MSC manufacturer and provide frozen MSCs for clinical trials evaluation to hospitals around Australia).
Then, following the finding of MSCs capacity to suppress the immune system, they also began clinical studies to evaluate their safety and effectiveness for treating transplant rejection. Their first trial, in 2007, was as the last resort for a young bone marrow transplant patient who was suffering the final (and usually fatal) stage of Graft vs Host Disease (GVHD). This may happen after a bone marrow transplant where the donor’s bone marrow attacks the patient’s organs and tissues, in serious cases with horrendous consequences.
Soon after infusion, the MSC’s calmed the immune reaction, reduced the symptoms and began repairing tissue. Subsequent treatments over the following weeks saw almost complete remission. Months later, the GVHD returned, but faded again with further MSC treatment. This cycle of remission and relapse continued for the next few years. Now in 2015, the patient has been free of GVHD for over three years.
Protocols for treating patients continue to be developed. For example, there is now a clinical trial with MSCs being administered as soon as the GVHD is detected, rather than waiting until the disease becomes life threatening. Subsequent GVHD trial patient recovery numbers show that MSCs can significantly reduce and even eliminate rejection (52% recovery vs 10-15% recovery rate before MSCs).
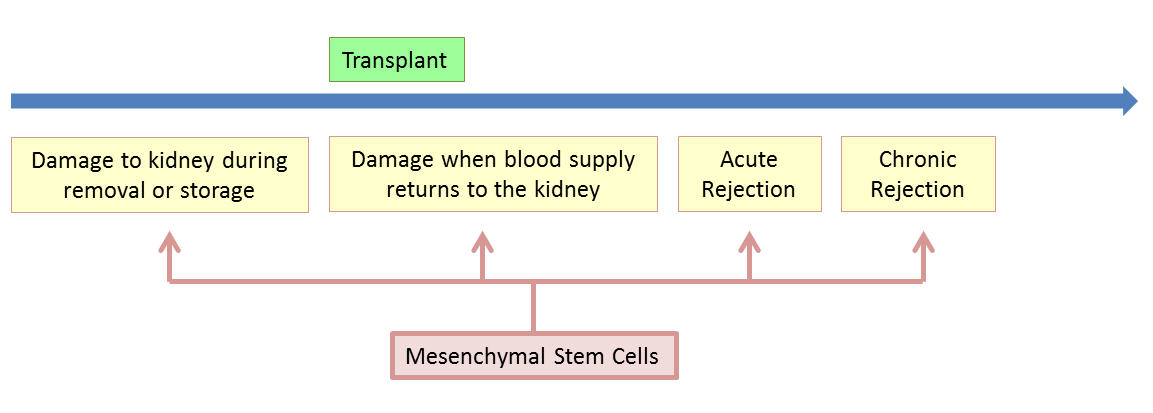
Two years ago the Centre began clinical trials on lung and kidney transplant rejection, and on repairing donor kidneys that have been damaged during removal, between transplants, or when blood supply returns to the kidney when first transplanted.
 A typical kidney transplant rejection treatment protocol consists of a series of small infusions (about 40mls) of MSCs into a vein, typically over a 4 week period: the rejection fades away.
A typical kidney transplant rejection treatment protocol consists of a series of small infusions (about 40mls) of MSCs into a vein, typically over a 4 week period: the rejection fades away.
While as yet incomplete, all of these trials have provided clear evidence of the effectiveness of MSCs in suppressing rejection and repairing damaged organs.
So what are we waiting for?
The paperwork. Every new drug treatment needs detailed written clinical trial evidence of safety and efficacy. In the right format, over an extended period, in triplicate.
Formal clinical trials are longwinded, meticulous beasts (as they should be, we don’t want the cure to be worse than the disease). They usually go through three phases before release:
- Phase I clinical trials test a small group of people (e.g. 20-80) to evaluate safety (e.g. to determine a safe dosage range and identify side effects). These are cheap to run and are often run in-house
- Phase II clinical trials may test from twenty to several hundred to check that it works as intended and to further evaluate its safety (the number depends on how effective the therapy is: these Phase II studies only need 20-66 patients)
- Phase III studies may test several hundred to several thousand by comparing the therapy to other therapies, monitoring for adverse effects, determining dosing schedules etc, depending on the design of the trial and expected response.
There is also a fourth Phase IV done after the treatment has been released for use. Where clinicians monitor the effectiveness on the general population and check for adverse effects of widespread use over longer periods of time, etc.
The current MSC kidney transplant rejection trials are in Phase 1. Phases II and III get progressively more expensive (we are talking several to many $millions) and time-consuming (3-5 years depending on the recruitment numbers). However, if the early Phase clinical trial outcomes demonstrate high clinical efficacy then it may be possible to fast track release (making it even less than 3 years).
So for those who want to be involved right now, it’s not easy. Patients may be recruited to a trial if they fit the profile and eligibility criteria (people who are actively rejecting a transplanted kidney and being located in the right city are two big ones) and are prepared to accept the risks. Some patients may be granted special/compassionate access to a trial, for example if the treatment is their last resort, having exhausted all other avenues.
So, in summary, MSCs look like they can be used to stop rejection in its tracks, but we need to wait for the clinical trial outcomes. While frustrating, this is a lot better than where we were a few years or two ago, when things looked positive, but unproven.
The light in the tunnel is getting brighter, but there are still a few stops before it arrives. For a working transplant, I can wait, and maybe even put off any transplant until it does.


