Empowering dialysis users and caregivers
Search for dialysis centres here
 Log in to explore the world's most comprehensive database of dialysis centres for free!
Log in to explore the world's most comprehensive database of dialysis centres for free!

Kamal Shah
Hello, I'm Kamal from Hyderabad, India. I have been on dialysis for the last 13 years, six of them on PD, the rest on hemo. I have been on daily nocturnal home hemodialysis for the last four and half years. I can do pretty much everything myself. I love to travel and do short weekend trips or longer trips to places which have dialysis centers. Goa in India is a personal favorite. It is a great holiday destination and has two very good dialysis centers.
E-mail: This e-mail address is being protected from spambots. You need JavaScript enabled to view it
India's patent laws - two sides of the debate

When I contacted Alexion Pharmaceuticals, the sole company in the world that manufactures Eculizumab, the only drug with which I can have a successful transplant, they said they had no plans to bring the drug to India. Their chief concern was India's weak IP protection laws.
In effect, they were worried that a local company could easily reverse engineer the drug and sell it at a fraction of the price. I was quite surprised that Indian laws would allow that. For a while, I assumed that they were referring to the illegal drug market where the drug would be copied in highly questionable conditions and sold illegally.
I was wrong. Indian patent laws allow reputed Indian manufacturers to reverse engineer drugs and sell them at a fraction of the price at which the original drug is sold by the company that actually invented the drug.
I read up a little on this recently. This issue was in the news after two significant rulings - on Novartis' Gleevec and Bayer's Nexavar, both cancer drugs. The rulings rejected the requests of these companies to prevent Indian companies from selling reverse engineered versions of the drugs at a fraction of the cost at which the originals were being sold.
There are a few things we must know. India used to provide only for process patents and not product patents. So, you could get a patent only for the way you produce a certain drug, not the drug itself. This changed in 2005, when due to India signing the WTO treaty required it to become TRIPS compliant which provided for product patents. However, some safeguards were provided which prevented MNCs from monopolising their products often to the detriment of the general public. It is often the interpretation of the safeguards that come up for litigation.
For example, there is a provision called Compulsory License where the country can allow a company to manufacture a generic version of a patented drug without the consent of the patent holder and sell it in the country by paying a certain royalty to the patent holder. Under what circumstances this can be done and what is the royalty that would be paid are all not specified clearly.
Look at all this from a big pharma company's point of view. They would believe that since they have the patent to the drug, no one must be allowed to sell it. In fact, the price at which Indian companies sell the drug is often a miniscule fraction of the manufacturer's price. Further, the cheaper version could also be exported to other countries and this could be disastrous for the patent holder! The pharma companies spend a lot of money on research and actually bringing the drug to the market. They believe that it is unfair to them to allow generic versions to be sold by someone else, at such low prices!
Fair point.
Now, look at this from a patient's point of view. There is a drug that is available in the market. The drug could save his life. But is priced so high that he cannot afford it. Or it is priced so high, his insurance / government will not pay for it. He would say this is completely unfair! He would argue that in the case of life saving drugs, commercial exploitation must not be allowed. When someone else is able to produce the drug and sell it much lower prices, this should definitely be allowed!
Again, fair point!
What is the way out?
... http://www.kamaldshah.com/2014/11/indias-patent-laws-two-sides-of-debate.html
A duodenum biopsy
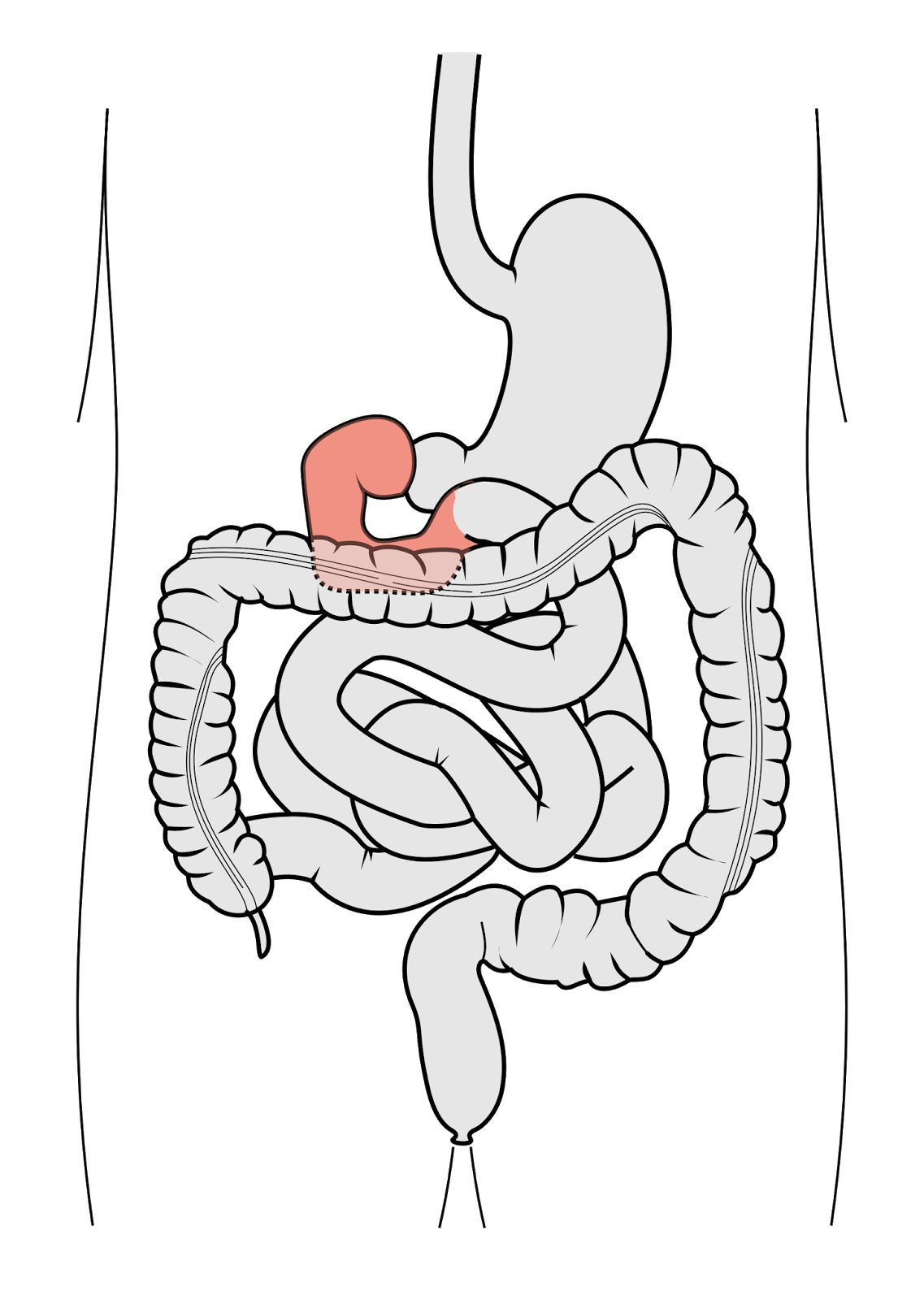
I have been having recurrent diarrhea for the past month or so. I am on my third antibiotic course. Everything seems to be ok for a few days and then it starts again. The day before yesterday, the gastroenterologist suggested that we do an endoscopy and a biopsy of the duodenum.
This sounded scary. Biopsy of the duodenum? Whatever did that entail?!
I have become an endoscopy veteran by now and have had more than I care to count. In fact, I stumbled upon this post where I actually compare how endoscopies have changed over the years! Just imagine! So, I wasn't in the least worried about the endoscopy. It was the other beast I was worried about. How can something called 'biopsy of the duodenum' be anything pleasant?!
Anyway, these days I have stopped thinking about all this, stopped applying my mind to my treatment and surrendered completely to the doctors. Its become a pointless exercise. So much of it is just trial and error!
So, I went ahead and got the endoscopy and the duodenum biopsy done. I was advised to do a heparin-free dialysis that night. A biopsy involved cutting off a tiny little piece of the tissue in the duodenum and examining it under the microscope. So, there was a small chance of bleeding. Heparin is the drug that is used for almost all dialysis patients to prevent the blood from clotting when it is outside the body getting purified in the artificial kidney. So, if you used heparin after a biopsy (and even a surgery), chances are that the site of injury will start bleeding.
It is normally fairly straightforward to do a heparin-free dialysis in-centre during the day. All that is needed is to flush the lines with saline every 30 minutes. At night, it can be quite a bother. Giving a saline flush every 30 minutes means someone needs to stay up the whole night. Guru, the tech who dialyzes me was, as usual, very co-operative. He stayed up the whole night and religiously flushed my bloodlines with saline every 30 minutes.
All in all, everything went off well. The biopsy report is expected in 4-5 days. Let us hope we get some clue on what the issue is.
... http://www.kamaldshah.com/2014/11/a-duodenum-biopsy.html
Only something that will prevent HUS recurrence can help me in the long run
However, I am not sure if that is entirely accurate. Dialysis, however much you get, can never replace all the functions of the kidney. There are some functions that it does not even attempt to replace. That is left to the medicines to manage. We unfortunately know so little about the human body that it is always an uphill task to manage such intricate mechanisms within the body with a bunch of tablets.
Only a transplanted kidney can give you close to normal body functioning. Things like Mineral and Bone Disorders (MBD) are very difficult to get a handle of. I have experienced this first hand. I am struggling with severe, debilitating bone pain from the past month or so, something which has been getting worse and we were not able to do anything to arrest it. Even seasoned nephrologists agree that MBD is something that they are just not on control of yet.
The trouble with me is my primary disease - Atypical Hemolytic Uremic Syndrome (aHUS). With this disease, the chances of recurrence after a kidney transplant are more than 90%! Which pretty much rules me out from getting one unless I get access to a drug that will prevent recurrence of the HUS.
There is a drug Eculizumab that is available in many countries that has been shown to prevent recurrence of HUS in transplanted kidneys. There is one more drug (Omeros 721) in clinical trials stage. Both these drugs are not available in India yet.
I just hope they become available before my MBD gets out of hand.
... http://www.kamaldshah.com/2014/11/only-something-that-will-prevent-hus.html
Modi government planning Universal Healthcare rollout in India
India currently spends about 1% of GDP on healthcare. China spends about 3% and the US about 8.3%. That is about to change. If things go as per plan, Prime Minister Narendra Modi's government is planning to rollout Universal Healthcare for India beginning April 2015. The project will be taken up in phases and would eventually cover the entire country by March 2019.
I have always been a proponent of Universal Healthcare. The erstwhile united Andhra Pradesh state had shown the way by implementing the dramatically successful Aarogyasri scheme where people who were below the poverty line (BPL) were given access to healthcare they could only have dreamed of in the past. Currently, of course, the number of beneficiaries of the scheme far exceed the number of people who were BPL as per the records. The scheme is being misused by people who are not the intended beneficiaries. Despite this, I would say the scheme is really good because the lives of thousands of poor people are being saved every year thanks to this scheme. The loopholes must be plugged and the scheme continued.
Modi's task would, of course, be far more challenging. For starters, however, they wouldn't have to worry about unintended beneficiaries getting the benefits of the scheme. There would be no unintended beneficiaries as the scheme is not restricted to BPL people. It is for all. Some might argue that this is not wise as there was no need to subsidise healthcare for people who could afford it. While this argument holds merit in the case of the super rich, ask any middle class family with someone on a chronic condition like dialysis and you would see how medical treatment can wipe out any average family's life's savings in just a few months.
The scheme is going to cost the government about $11.4 billion annually. To put this number in perspective, India spent $47.4 billion on defence in 2013. So a fourth of that for Universal Healthcare is a good bargain, if you ask me!
The plan is being thought through well. Primary healthcare will continue to be offered by the Government especially in rural areas where infrastructure is going to be improved. Tertiary healthcare is going to be offered through the insurance model. The scheme includes some basic drugs and diagnostic tests free.
While reaching the entire country in an effective way will obviously take decades (which is not surprising since it involves a sixth of the world's population!), we must not shy away from this basic necessity of the people due to this. A beginning has to be made somewhere.
I have always maintained that access to healthcare should be a fundamental right. No citizen of the country should be allowed to suffer if a treatment is available just because he or she cannot afford it.
Dr. Martin Luther King, Jr had once said, "Of all the forms of inequality, injustice in health care is the most shocking and inhuman." Let us not allow this injustice in health care to continue for much longer in our country.
... http://www.kamaldshah.com/2014/11/modi-government-planning-universal.html
When talking about the dialysis diet was called 'vulgar'

I was talking to a group of dialysis patients a few months back. I first did a general talk about how to have a good quality of life despite being on dialysis. I then had a Q&A. Typically, questions in this kind of a session invariably turn towards the diet. Diet, for most dialysis patients, is the worst problem if you don't count fluid restrictions.
I was answering some of the general questions on diet when a gentleman, probably about 60 years old started shouting. His contention was that any talk about things like diet was totally unnecessary and he even called it vulgar. I was quite taken aback. He said his wife was on dialysis and their entire life's savings have been spent on her treatment. The anger in his voice was palpable. For him, any talk that purportedly gives support to dialysis patients should only be about how patients should work together to get the government to subsidise dialysis or even make it free.
I explained to him that while I understood the financial problem of dialysis patients and their families, for the patients, diet is a big problem. Addressing the financial issues was going to take time in a country like India because a huge, concerted effort from patients, families, providers, doctors etc. would be needed and the process would be very slow. In the meantime, what was wrong in patients getting some queries answered on their diet and other simple things that could make their life better?He softened up after this.
I could totally understand his problem though. While in developed countries, patients don't need to think about how much their treatment costs, in India, treatment options are primarily dictated by ability to pay. When patients are often wondering how long they would be able to continue dialysis, talk about diet, exercise, quality of life etc. may appear vulgar!
When I talk about more frequent dialysis, I realise that a large number of patients would do it if they could afford it. When the constraints are not in your control, what really can you do?
Honestly, I was quite shaken up by the gentleman's outburst. Their life probably turned upside down after the diagnosis. All their plans probably went haywire. He needed some place to vent. He obviously couldn't vent in front of his wife. I am at least hoping that he didn't do that! A guilt trip is the last thing a dialysis patient needs!
This is why I am fully supportive of any attempt at Government sponsored healthcare. We need to eventually get into a mode where an individual gets the treatment he or she needs without having to worry about where the money for this is going to come from.
... http://www.kamaldshah.com/2014/12/when-talking-about-dialysis-diet-was.html

